WORLDS APART: Dr. Jason Cundiff

BY VAL SCHOGER PHOTOGRAPHY BY MIKE FENDER / PHOTO DOCUMENTATION OF MISSION TRIPS BY MAREK LICHOTA[dropcap]W[/dropcap]hen an earthquake struck Haiti in 2010, news reports showed thousands of injured victims. “I remember thinking, ‘I have got to get down there,’” Dr. Jason Cundiff says. An estimated 160,000 people had been killed, landmarks and cities were destroyed. Many hospitals had collapsed and existing medical providers could not keep up with the number of victims and severity of injuries. He knew he could help save lives.

At the time, Dr. Cundiff worked as a general surgeon specializing in trauma and robotic surgery at Yakima Regional Medical Center in Washington State and had extensive experience with trauma patients. He immediately reached out to several large non-profit medical relief organizations, but his passionate “I’m ready to go” was met with stiff regulations and bureaucracy. He had all the qualifications, but the accreditation process would take months. The next day, a newspaper article caught his attention. A local church called for volunteers, hoping to turn their planned yearly mission trip of providing dental care in the Dominican Republic into a medical relief trip for the earthquake victims in Haiti. This time, his call and offer to help was highly appreciated—it set his first medical relief trip in motion.
“Within 72 hours we had the team together. The church had the financing already in place and the tickets booked. I was able to get the necessary instruments and we packed our bags.”
Within a few days, Dr. Cundiff as the lead surgeon and a team of other experienced healthcare professionals boarded a plane to the Dominican Republic and from there continued on a road trip to a clinic in Jimanì, a town at the border to Haiti. He remembers there were hundreds of severely injured patients in makeshift beds in a field outside the clinic. The patients refused to go inside the building, terrified that an aftershock could cause it to collapse and trap or bury them. Medical teams from around the world had come to provide medical care.

Dr. Cundiff’s team was set up in an operating room, working 14-hour shifts. “I was worried whether we could provide quality work and employ the same standard of care as in the U.S., and realized as long as we had air control and sterilization, we could do the same surgery that we were doing back home. It just came down to the patient and the problem. Let’s fix it. Let’s get to the next patient. So, the experience really brought me back to the base aspect of medicine.”
The U.S. medical team saved hundreds of people and the patients’ gratitude made a lasting impression. “To have a bunch of strangers show up in their greatest moment of need, it really meant something to the Haitian people. An amputation is never a happy operation, but I could not believe the optimism and positivity from these patients, who were just happy to be alive and get themselves back to living. It was an incredible experience.”
When Dr. Cundiff returned home, he realized the huge impact a small, capable medical team could make. “There are not many flexible and self-sufficient surgical outreach organizations, but there are millions of people who have to live with health conditions that will worsen if left untreated,” he explains. Determined to continue the work, he founded Pacific Northwest Surgical Outreach (PNSO), a 501(c)(3) charitable organization. Since then, he and a group of anywhere from 9 to 15 healthcare professionals have ventured to remote areas in the poorest countries in the world, providing surgical procedures to those who have only a little access to medical care.
According to a yearly monitoring report published by the World Health Organization (WHO) and World Bank, half of the world’s population of 7.3 billion people cannot obtain essential health services. The WHO identifies and monitors countries that have insufficient access to health care, and, in partnership with governments and other organizations, offers strategies for global health concerns. Organizations such as Doctors Without Borders, Oxfam, Samaritan’s Purse, the Red Cross, Partners in Health, and many other charitable efforts focus on primary care and deploy surgical teams to assist during catastrophic events when there is an influx of trauma patients.



For the medical team at Pacific Northwest Surgical Outreach, providing specialty surgery is the primary focus when they venture to remote areas of this world. PNSO helps patients with dire medical conditions who have been rendered unable to live a normal life, with medical problems that can be solved with surgery. Carefully assessing the patients’ overall condition, PNSO can help those who are healthy enough for surgery. The most common procedures provided are the removal of growths and tumors, the repair of hernias, and the removal of gallbladders.
Once PNSO completed its first missions, there was a snowball effect. “People started contacting us and telling us about areas in need,” Dr. Cundiff remembers. “Those callers are often relatives or friends of people who are serving in organizations that are already on the ground, mostly faith-based organizations. Our first step is to figure out if we can do surgery in the particular location. I have operated in tents before but for the best results and to be able to operate all day, we prefer a room with closed-system air conditioning. We can bring most of the other needed tools and supplies.”

Before the mission, PNSO ensures a minimum of 50 patients will be scheduled and lined up for screening by the time the team arrives on location. With so many countries underserved worldwide, the process of picking a location requires careful review. One of the determining factors, and an aspect PNSO will not take chances on, is safety. “If there’s any question of instability or unrest in a geographical area, then we will not be able to travel there. South Sudan was very stable when we went at that time. We’ve never felt unsafe. It wasn’t until the rebellion in 2013 that the place became unsafe. The organization that sponsored us there, South Sudan Outreach Ministries, contacted me in the last month to let me know that the rebels are gone.”
South Sudan is the youngest country in the world. Its size is comparable to the size of Texas and the population is an estimated 12 million people. When PNSO planned their first trip to South Sudan, the governor of the area, a Dinka tribesman, informed them there were only 30 surgeons in his entire country.
With 13 completed relief trips since 2011, Dr. Cundiff and his fellow humanitarians have overcome hurdles they could have never anticipated. The first time they arrived in the small clinic in Morobo County, South Sudan, the group was surprised to find the operating room bare of any furniture. There was no operating table. When the team entered the room the next day, a hand-crafted operating table was set up for them. Admittedly, it looked different, but it matched the height and width specifications exactly. It turns out that South Sudan has large forests and excellent craftsmen. The operating table was manufactured overnight from a large slab of solid mahogany wood by local artisans, courtesy of PSNO’s host organization.
PNSO volunteer Amanda Popish, a second-year medical student at the time, describes her experience in Uganda in 2016 on PNSO’s website: “It took no more than a few minutes off the plane to realize what the theme of the trip (and, I would imagine, many trips to Africa) would be: ‘roll with it.’ Getting to baggage claim and realizing that two surgery bags filled with surgery supplies had gone missing set the tone. We had lost surgery bags, we had nights where technical difficulties made it impossible to clean instruments, we had three hundred people waiting in the Uganda heat in June to get seen with only four or five medical students to screen [them]. But there couldn’t have been a team more ready to roll with it than this group. … On a personal note, I would add that there have been few moments in my life that left me as wide-eyed and exhilarated about my future as I routinely felt throughout this trip. … I could never have imagined getting the exposure and opportunity to learn, connect, and dive-in quite as hands-on as this experience allows. I am so deeply grateful to PNSO for what it has given me, and what it continues to give the world.”
The program touches the lives of all its volunteers, and especially the medical students take away an experience that will stay with them for the rest of their lives, often propelling their medical careers.

Everyone is eager and happy to actively contribute to the group effort and prep work. “We have it down to a science,” Dr. Cundiff says. “We take sutures and drapes and everything we need for the particular operation. So, if you are going on the trip, you can bring your own carry-on with whatever you want for clothes, but you will need to check-in two items for PNSO. The one item I do not trust checking in is the electrocautery. It was donated to us and was previously used, but it works great. It weighs about 40 pounds and so, I fasten a strap to it and take it aboard with my carry-on.”
But the team cannot provide all of the necessary items. Supplies such as IV fluids and oxygen must be provided by the host organization or will require additional logistical efforts from the volunteers as they are not permitted on the plane. All other supplies, suction machines, disposable supplies, and small generators that have never been used and weigh less than 50 pounds are lugged in by the volunteers. PNSO also transports medications but this has become more difficult in recent years. “The DEA was very helpful. We could bring anything we wanted on the earlier trips. And then about three years into it, the rules changed, and we were unable to bring narcotics. But we can pack our own antibiotics and all non-narcotics in controlled doses. We usually have a physician on the ground who can come in and provide the sedatives for anesthesia,” Dr. Cundiff explains.
 The medical relief missions certainly require a special set of skills beyond medical training. The contrast between Dr. Cundiff’s regular work could not be more pronounced. In a hospital setting in the U.S., he conducts most of his operations with the DaVinci Surgical System, a high-tech computerized robot that promises smaller scars, shorter recovery times, and fewer complications. This surgery tool requires an initial investment of around $2 million from the hospital, and patients have the choice to elect this particular type of operative tool.
The medical relief missions certainly require a special set of skills beyond medical training. The contrast between Dr. Cundiff’s regular work could not be more pronounced. In a hospital setting in the U.S., he conducts most of his operations with the DaVinci Surgical System, a high-tech computerized robot that promises smaller scars, shorter recovery times, and fewer complications. This surgery tool requires an initial investment of around $2 million from the hospital, and patients have the choice to elect this particular type of operative tool.
In contrast, some of Dr. Cundiff’s patients in developing countries have never seen a physician. While most of the electronic equipment he uses during missions might not be the latest model, it is field-tested and reliable.
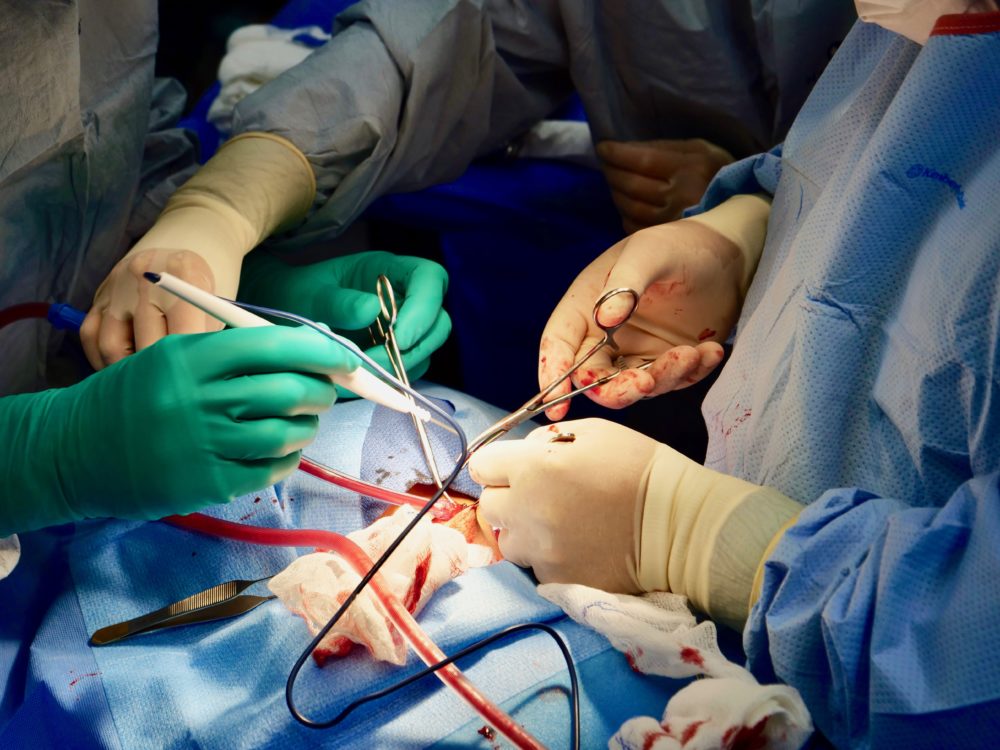
It’s amazing to see the transformation—PNSO arrives with a truckload of bags at a location in one of the world’s poorest countries, and within a few hours they will have a tent or a regular room converted into a fully functional surgical room. Dr. Cundiff points out that he will not use any sub-standard equipment, but that in some situations, he needs to be resourceful.
A video documentary from the second trip to South Sudan shows him using sterilized garden shears to cut a bone protruding from a patient’s thumb. With the thumb badly infected and the danger of losing the entire hand, the garden shears were an effective solution.
In 2018, Dr. Cundiff moved to Panama City, Florida with his wife and three-year-old daughter. His wife, a nurse who has been on several missions, is originally from New Orleans and has always had the dream of living on the Gulf Coast of Northwest Florida after many family vacations as a child. Today, Dr. Cundiff works as a trauma and general surgeon for Bay Medical Sacred Heart hospital where he specializes in minimally invasive surgery. He has started a sub-chapter for PNSO, Panama City Surgical Outreach (PCSO), in Northwest Florida.

According to Dr. Cundiff, there is no central network that connects small organizations and medical providers. Except for his first trip to Haiti, all of PNSO’s missions have started by word-of-mouth. “People heard what we do and someone knew someone who worked with a small church group in Moboro, South Sudan, and desperately needed a surgeon. That was our next trip. South Sudan happened like that; Uganda, Peru, Guatemala, and a subsequent trip to Haiti came about that way.”
Relief trips are organized six months in advance, and the next trip planned is to Sierra Leone in Western Africa in June 2019. “This time, it’s going to be at a small hospital that doesn’t have any staff,” he says with a smile. “There are thousands of patients in the area. We are probably going to be overrun.”
This statement exemplifies Dr. Cundiff’s endless optimism and his fearless “we will get it done” attitude. Whether he’s on home turf focused on the training-intense DaVinci system with its high-resolution monitor and silicone finger adapters that are virtually connected to a steady and precise robotic arm, or operating on patients whose language he doesn’t speak, in a non-climate controlled room, with the most basic equipment in the middle of nowhere in a place not even listed on a map, he seems to be in his element.
But how is it possible for him to excel at these two seemingly opposite ends of the spectrum? Dr. Cundiff doesn’t believe the two are so different after all, and there’s a method behind all his success. He explains, “I’m okay with situations that are out of the ordinary and I’ve always been good at it for whatever reason. I am a mountain climber, and there is a method to reaching the summit. You take rest steps to conserve energy, and you focus on the next task ahead of you. It’s the same with surgery, whether you are working with a high-tech robot or working with very basic equipment and a team that works together seamlessly. Take small steps, focus on one problem at a time, set priorities. I approach surgical problems systematically, like mountain climbing, with small rest steps.”
[divider]Q& A with Dr. Jason Cundiff, founder of Pacific Northwest Surgical Outreach

How do you ensure the patient’s wellbeing after you have returned home?
If somebody has a complication after the surgery, we have arrangements with the nearby clinic. We would pay for anybody to be brought to that hospital if they had complications. Knock on wood, that has never happened. But everywhere we go, we make sure there will be good follow-up care. So, as long as you use good surgical technique and you rinse your wounds really well and administer antibiotics, which we all do in all the cases. We have not had one serious infection and we’ve done more than 500 operations over the years.
Have you ever had a situation that got out of hand?
During surgery, we have never had an airway problem or a code blue or anything like that. We make sure that our patients will be fit for surgery, and screen and assess their overall health. If somebody comes in and their medical condition seems a little debatable, we will have to tell them that it will not be safe for the procedure. I think that’s why we’ve done so well.
Have you ever found yourself in a dangerous situation in any of the countries your team worked in?
People can get upset if we tell them we cannot perform the surgery. We actually had somebody come back with an AK-47 in South Sudan because we wouldn’t operate on his mother. He threatened the team that was taking care of us. His mother was clearly a very sick woman and we would have probably done more harm than good. He was arrested by the authorities. But that was an unusual thing to happen.
How are PNSO and PCSO funded?
We have had equipment donated and the team comes together to organize fundraisers. Back in Washington, we are having the “Ragin’ Cajun Shindig.” It’s our biggest fundraiser, with Cajun food and a live auction. In southeastern Alaska, a few of our friends are raising funds for us by organizing small events. We were planning on having a duathlon race here in Panama City Beach.
Depending on the success of the fundraising efforts, all mission participants might have to contribute to their traveling expenses and contribute to the purchase of the airfare. Everyone contributes and we are very grateful for that.
What expectations do your team members have?
We have been in the jungle of the Amazon in Peru, to the highlands of Guatemala, the coastal areas of Haiti, and our team members have different skill sets and are in different stages of their careers. We have seasoned surgeons and anesthesiologists, but also pre-med students.
I tell everybody when we have our big pre-meetings, “This is not going to be what you expect either way, but it will be a phenomenal experience for you. So, one way or another, it’s going to change your life. But you have to remember, leave your expectations at the door, because they’re going to be filled in ways you don’t expect.”
I don’t think I’ve ever had anybody say, “I wish I didn’t go on this trip.” It’s not something that many people can do on a regular basis, because they have lives and families for vacations. But the people who can come, have come over and over and over and we actually have difficulty sometimes because there are too many people who want to go.
 What were your most gratifying experiences?
What were your most gratifying experiences?
There are so many patients and success stories. In South Sudan, we had a 25- to 30-year-old guy. He had a growth on the top of his foot about the size of an orange. I think it was a ganglion cyst that had never been treated. He had this sneaker that must have been 10 years old with the tongue cut out to accommodate the cyst. He could not wear normal shoes. I was able to remove the growth and it closed really nicely. I actually wore the same shoe size, roughly, so I gave him my extra pair of sneakers. He was so unbelievably happy. When you watch our video documentary of our second trip to South Sudan, you will see several people who now have a new chance at life after they received surgery.
What was most unexpected during the relief work?
It felt like a miracle when we arrived at the border of Haiti after dealing with so many obstacles. We helped save hundreds of lives in the ten days we were there. Our most critical patients could be transferred to the U.S. Navy hospital ship USNS Comfort by Sea Stallion. I rode on one of the drop-offs and it was one of the most exhilarating experiences of my life.
What are you bringing back to the U.S. and our community in Bay County, Florida, from PNSO’s humanitarian missions?
Everything is so much more capable here in the U.S., but I just feel like my perspective and how I look at situations and frustrations has been altered through the experiences. I realize that many of my perceived problems are first-world problems. But as far as bringing anything back to the community, that’s a hard question.
Anyone who comes on the trip comes back with a different perspective. Ninety-nine percent of most types of procedures I do in the U.S. is robotic-assisted minimally invasive surgery. There’s still a need to do big open surgery on occasion. The mission trips allow me to focus on open hernia repairs and gall bladder operations. I probably do more open hernia operations in a week’s time in Africa than I do in five years of practice back in the U.S. And so, one of the things that these trips provide for me is a revamping of my clinical skills. It keeps me really sharp with those kinds of operations.
You worked at Bay Medical Sacred Heart hospital during Hurricane Michael. Did you feel reminded of your work with PNSO?
The emergency room at Bay Medical Sacred Heart was open and helped patients throughout the entire time during Hurricane Michael. I lived and worked in New Orleans during Hurricane Katrina, which was good preparation— I worked at Charity Hospital at the time. But that’s yet another long story. I think Hurricane Michael and the traumatic experiences that we had to go through have reminded us what’s going on in the rest of the world.
Find out more about Dr. Cundiff and
Pacific Northwest Surgical Outreach online: pnwso.org
PHOTO GALLERY